There are vein injuries and … vein injuries. Do you want to know how to deal with IVC or common iliac vein injuries? See here. And here. Occasionally, there are cases where you will need a different approach. Look at the following case. An 84-year-old male patient is being operated on for rectal cancer, having an abdominal-perineal resection. The phone rings and someone is telling you that there is an uncontrolled vein bleeding on this patient. “Can you please come and give us a hand?”
You get into the theater, scrub in and stand at the left side of the patient in front of a midline incision. The bleeder is on the bottom of the pelvis just on side of the rectum. The area is packed with swabs that have temporarily stopped the hemorrhage. It is not possible to see exactly where the bleeding comes from. If you remove the packs, a pool of dark blood fills the area and you are unable to see and do anything. Obviously, a big vein (probably the internal iliac vein or a major branch) has been damaged. What can you do?
A way to go is to temporarily reduce the bleeding and then try to make the venous repair. And how can you reduce the bleeding? By reducing arterial bleeding in the area. Read below to learn how to do it.
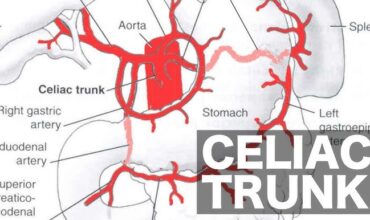
Let the pack in position, and dissect the common iliac arteries. Ask the anesthetist to give the patient 5000 IU of heparin (!!) bolus and get prepared to lose blood. He should bring blood from the blood bank in the theater and have normal saline bags ready to fill the patient. Ask the scrub nurse to prepare a second suction and find a pair of nice vascular clamps (or aortic clamps). Get a nice and long needle holder. Find the proper vascular stitches, like a polypropylene 3/0 with a 26 mm or better a 31 mm long curved needle. And now what?
First, clamp both common iliac arteries. Then, carefully, remove the packs. When you notice the bleeding area, put the two suctions just opposite to the bleeding point, keep them there still, and let them suck all the blood that is coming out. Be sure that the suctions are in the best position to let you see where the bleed comes from. At this moment the anesthetist needs to support the patient with iv fluids (normal saline in rapid infusion or blood). Keep calm. Forget about the bleeding. You have to focus just to put a couple of nice stitches across the lesion. Grap the vascular stitch with the long needle holder and put a stitch across the area where you think the bleeding point is. DO NOT PULL THE STITCH UPWARDS. Just put another stitch across the bleeding point on a figure of eight fashion. At this point, you can gently pull up the two ends of the stitch. If needed you can put another or more stitches across the bleeding area. When you are happy, tie up the stitch. Release the vascular clamps. Theoretically, the bleeding is now controlled. Put a couple of hemostatic gauzes close to the bleeding point and press with a dry swab on the top for some minutes. You can additionally rinse the area with warm normal saline. Check the patient for femoral pulses, to be sure that nothing has happened with the patient’s lower limb arterial flow after the removal of the clamps. If the femoral arteries are pulsatile you can say goodbye the let surgeons carry on their procedure…
This has been a real-life scenario. Yesterday, we operated on such a patient. I was called by my friend DK, general surgeon who had this complication during the case described above, in a district hospital. The bleeding had not been controlled despite two attempts, the first during the initial procedure, and the second attempt on the following day during an exploratory laparotmy after the bleeding had been packed. The bleeding was packed again , the abdomen was temporarily closed and the patient remained intubated in the ward. I went to give a hand the following day, together with my friend and colleague EP, vascular surgeon. We did exactly what is described above. And it did work.