The Palma procedure, a femoral–femoral venous crossover bypass using the great saphenous vein, is often considered a relic of the pre-endovascular era. With the widespread success of iliac vein recanalization and stenting, open venous reconstructions have become increasingly rare.
Yet there remain situations where endovascular options reach their limits—and in these moments, the Palma procedure can prove invaluable.
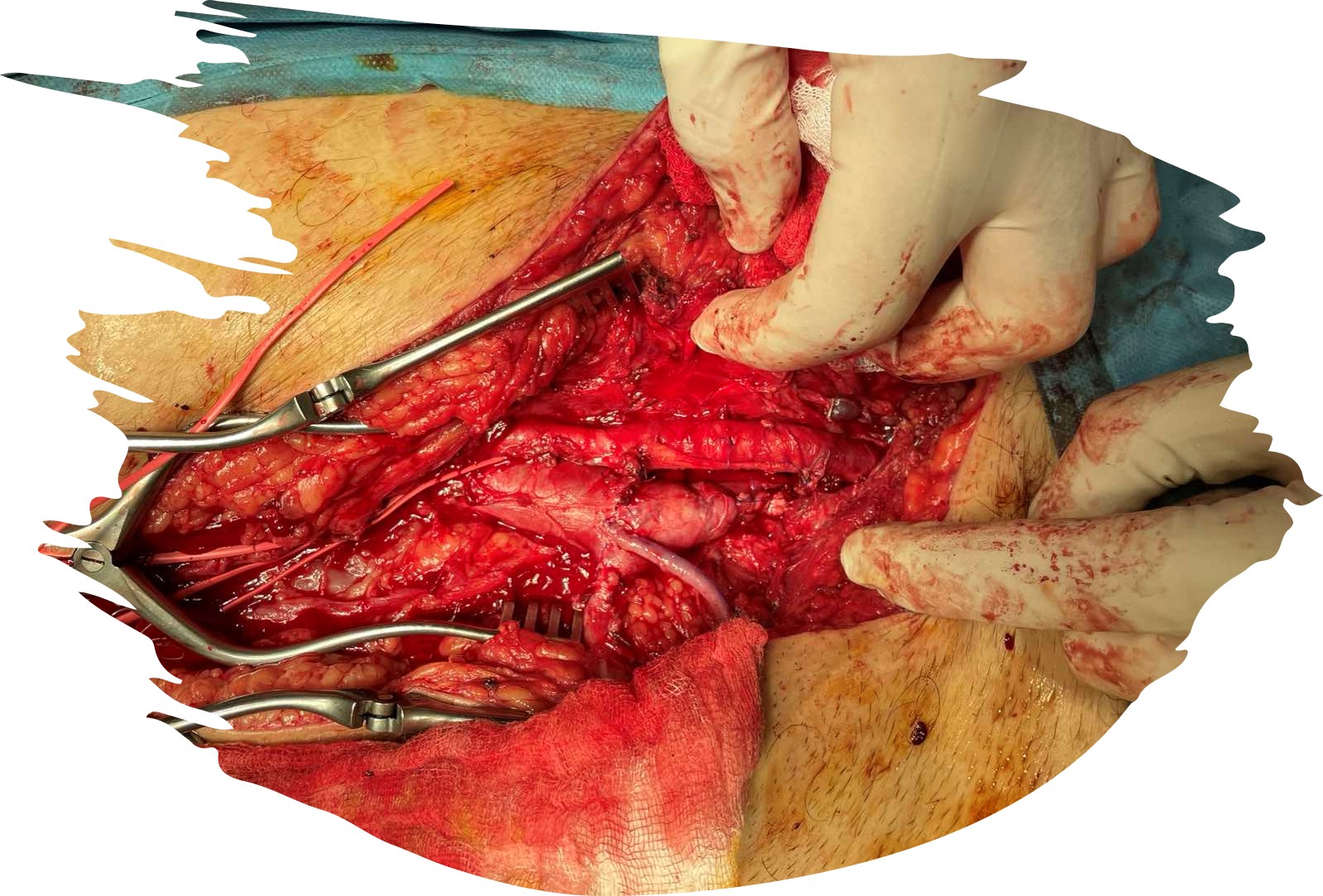
Recently, we came across such a case. The patient presented with a massively distended right femoral vein, the consequence of a long-standing arteriovenous fistula (probably congenital and not a post-traumatic as initially thought, with lots of arteriovenous communications), with nearly all tributaries already ligated when trying to repair. Complicating matters further, the external iliac vein was chronically occluded and entirely non-recanalizable endovascularly. Open venoplasty was neither an option as the chronically occluded vein had almost vanished.
Disappointed by the lack of any simple bailout, a flash came to mind: let’s try a Palma procedure.
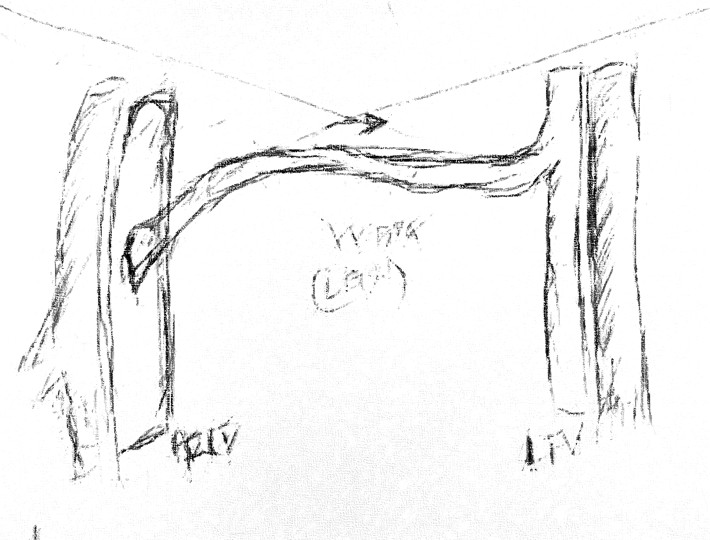
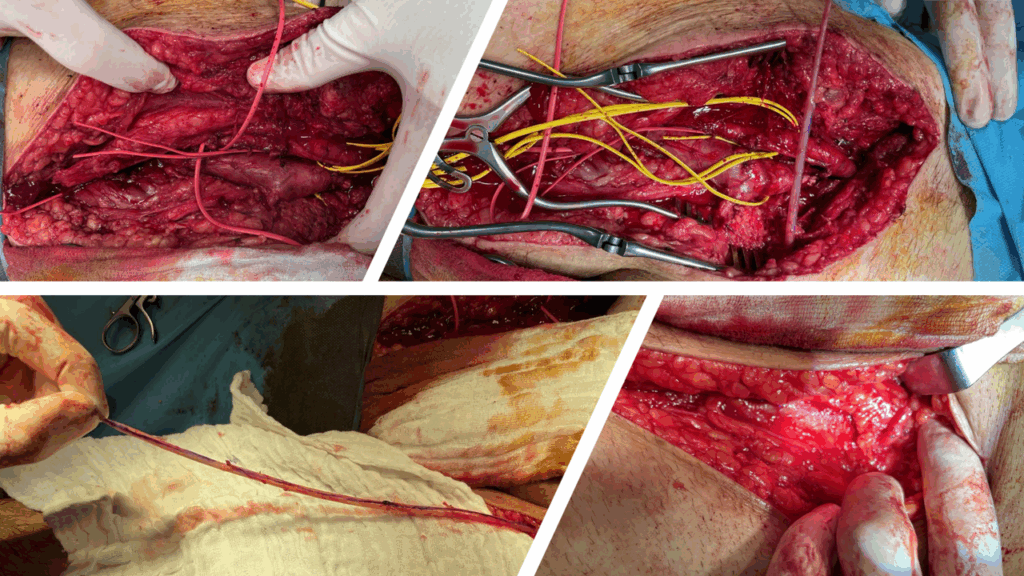
After rescrubbing the patient, we dissected the proximal contralateral great saphenous vein, mobilized it, and transected it at mid-thigh. The conduit was then tunneled subcutaneously across the suprapubic region to the opposite groin and anastomosed end-to-side onto the markedly dilated femoral vein.
Total operative time? Less than 45 minutes.
Physiological result? Immediate redirection of venous outflow to the contralateral iliac system.
This case is a timely reminder: although rarely used today, the Palma procedure still has its place. When endovascular recanalization fails or is simply impossible, this “old” technique becomes a beautifully simple and effective solution—old, yes, but certainly not obsolete.
Some technical tips?
- Avoid twisting of the vein graft. The great saphenous vein is long and easily rotated during tunneling. Carefully mark the vein before harvest or orient the adventitial surface to ensure correct alignment. Even a subtle twist can compromise flow and endanger patency.
- Consider creating an arteriovenous fistula to increase flow. A temporary or pre-existing arteriovenous fistula can significantly augment flow through the venous bypass, improving early patency—especially when the conduit is small or when inflow is borderline. In our case, the fistula already present played a beneficial role in driving flow across the crossover graft.