
An 84-year-old male patient with diabetes mellitus presented with a toe ulcer — a typical manifestation of chronic limb-threatening ischemia.
In diabetic patients, tissue loss in the foot is rarely the result of a single arterial lesion. The disease is usually multilevel, often involving the femoral bifurcation, the superficial femoral artery, the popliteal segment, and the tibial vessels. In this setting, restoration of adequate inflow is a fundamental step. And among the vessels that must not be underestimated, the profunda femoris artery has a central role.
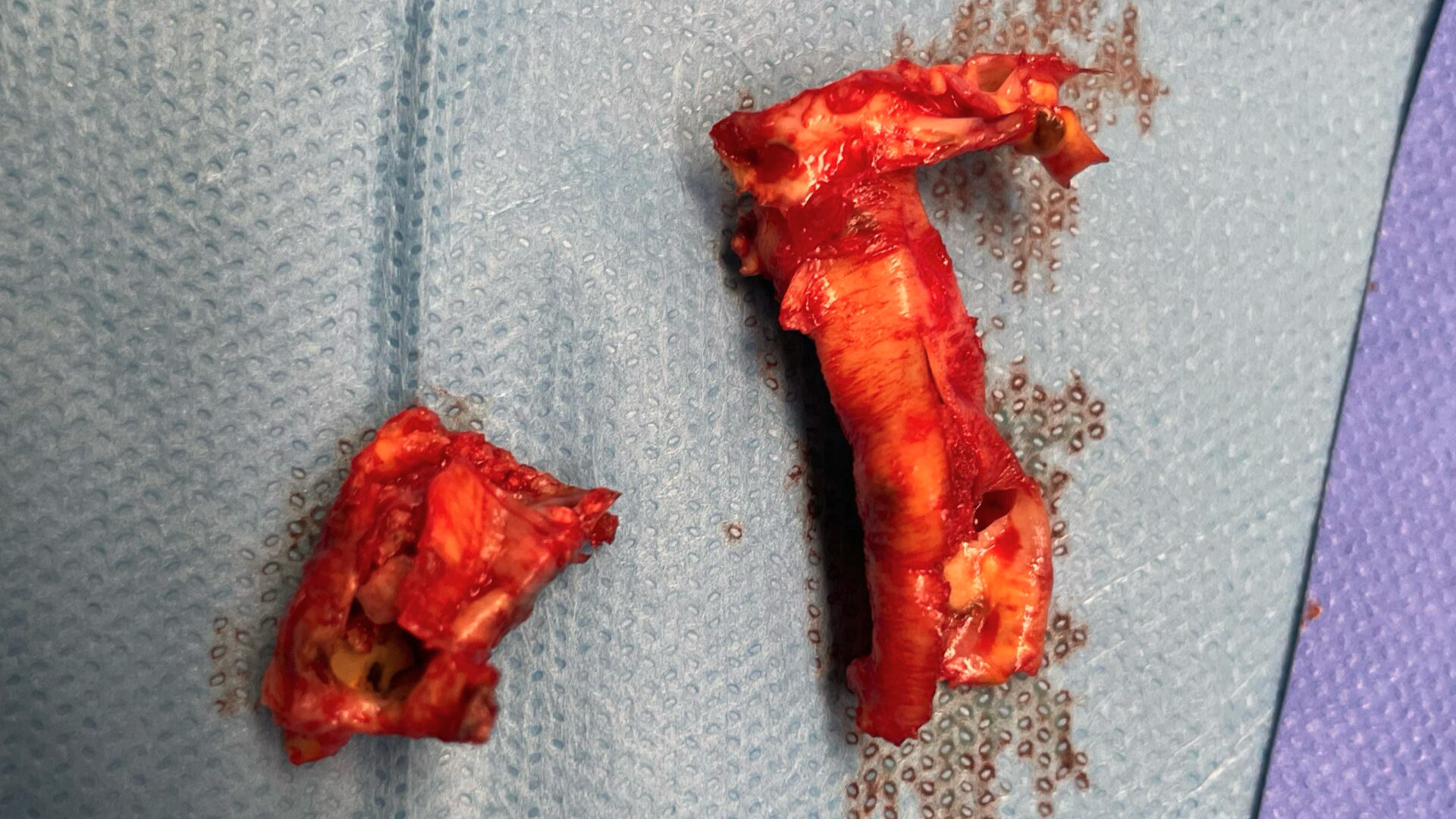
In this case, surgical exposure of the common femoral artery revealed extensive atherosclerotic disease involving the femoral bifurcation and extending toward the origin of the profunda femoris artery. A bulky plaque was removed by endarterectomy. The specimen clearly demonstrated the severity of the disease and the involvement of the profunda origin.
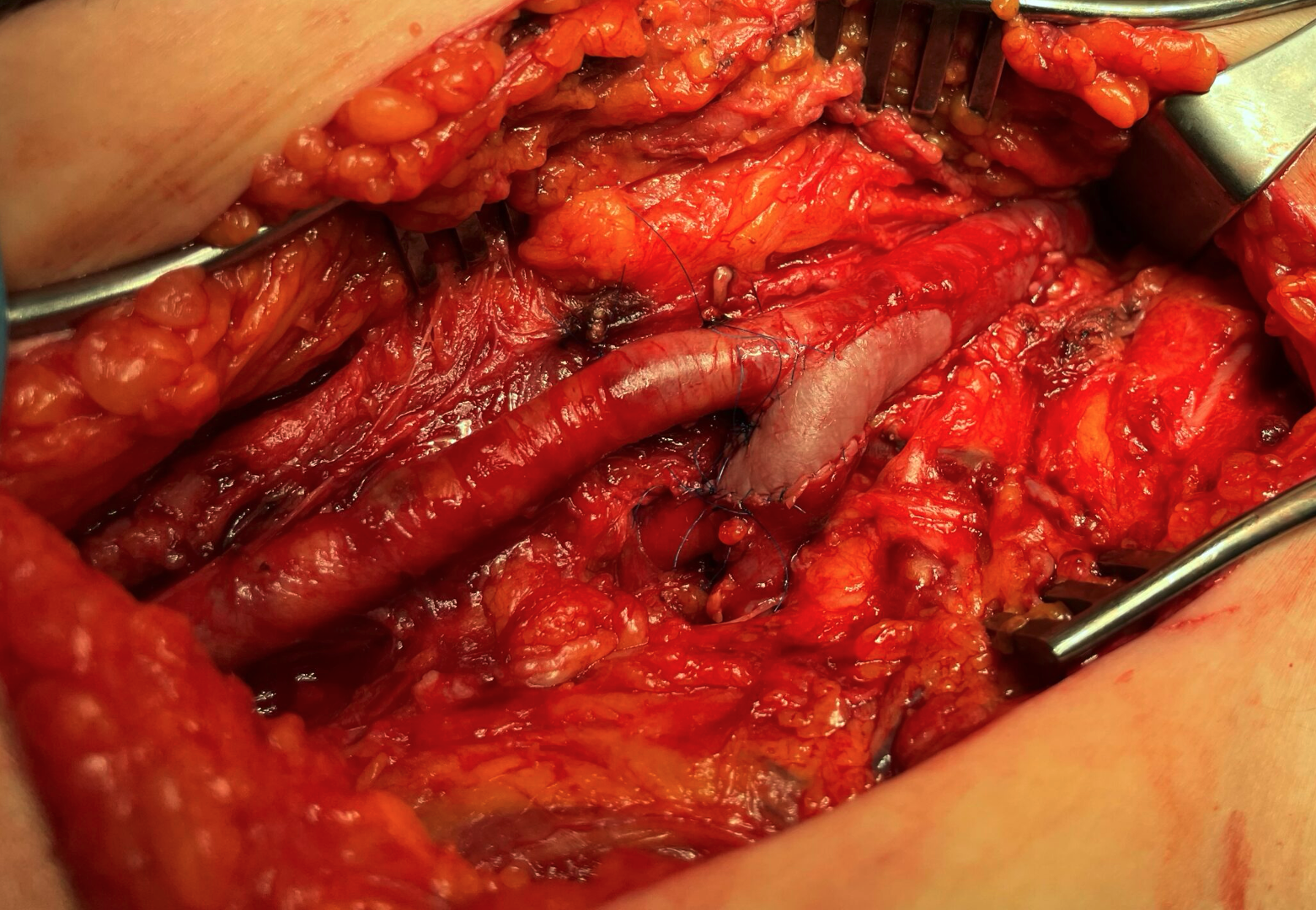
Reconstruction was performed with bovine pericardial patch angioplasty. The patch was extended toward the profunda femoris artery and ended at the profunda bifurcation, ensuring a wide and unobstructed outflow channel.
This technical detail is important. A limited common femoral endarterectomy may restore flow in the common femoral artery, but if the profunda origin remains narrowed, the reconstruction is incomplete. In patients with chronic limb-threatening ischemia, especially when distal disease is present, the profunda femoris may be the most important collateral pathway to the limb. Optimizing profunda flow can improve perfusion of the thigh and leg, support distal collateral circulation, and provide a stronger inflow source if further distal or endovascular treatment is required.
The surgical principle is simple: do not stop the reconstruction too early. The arteriotomy and patch should extend as far as needed to achieve a satisfactory endpoint and to fully restore the profunda femoris origin.
Femoral endarterectomy remains one of the most durable open vascular procedures. In the era of endovascular-first strategies, it is sometimes easy to underestimate its value. However, in selected patients, especially those with bulky calcified disease of the common femoral artery and profunda origin, open endarterectomy with patch angioplasty remains an excellent and reliable solution.
In diabetic limb salvage, the profunda femoris is not just a branch. Very often, it is the vessel that makes the difference.
Technical tips worth adding
A few technical details are worth emphasizing.
- Adequate proximal exposure of the common femoral artery is essential. The dissection should extend proximally under the inguinal ligament, toward the distal external iliac artery, up to the level where a good pulse can be clearly felt, confirming satisfactory inflow. After endarterectomy, invasive pressure measurement from the reconstructed artery and comparison with the systemic arterial pressure can provide objective confirmation that inflow has been adequately restored.
- Distally, exposure should allow adequate control of the profunda femoris beyond the diseased segment. The arteriotomy must be extended until a healthy distal endpoint is reached; stopping too early may leave residual plaque or an intimal flap at the profunda origin. If the distal endpoint is not perfectly smooth, fine tacking sutures may be necessary.
- The patch should be long enough to cover the entire arteriotomy and should be tailored to avoid narrowing of the profunda origin.
- Before final closure, good back-bleeding from the profunda and the superficial femoral artery should be confirmed. In selected cases, completion assessment with Doppler, duplex, or angiography can help exclude a residual technical defect.
The operation is finished only when the profunda femoris is truly open, not simply when the common femoral artery has been patched.