Occlusion of the infrarenal aorta is not uncommon, often occurring at or just below the level of the lowest renal artery. Is it distinct from the more typical pattern of diffuse aortoiliac stenosis? I believe it is, particularly regarding the approach for open treatment and the configuration of synthetic grafts. But let us start from the beginning.
- Incision: I prefer a midline incision for individuals of average body weight. It is not as lengthy as the incision required for open abdominal aortic aneurysm (AAA) repair, which usually extends from the xiphoid process to the pubic symphysis. Instead, it is a shorter incision starting at the xiphoid process and ending about 2 cm below the umbilicus. In obese patients with a large abdomen, one might consider a left retroperitoneal approach as an alternative, although accessing the right groin can be challenging.
- Approach: The standard transperitoneal approach is recommended on the left side of the duodenum and small bowel. The inferior mesenteric vein can be preserved or divided, depending on whether it obstructs safe access to the aorta. It is essential to identify and preserve the left renal vein as well. The dissection should extend just slightly below the aortic bifurcation; there’s no need to dissect beyond this point.
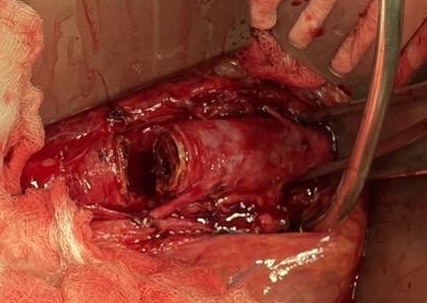
- Aortic Control and Clamping: I believe that the aorta should be thoroughly dissected free up to the level of the renal arteries and even a bit further upwards, if necessary, to accommodate supra-renal clamping if required. However, clamping the aorta at this level is not always necessary. In fact, an initial approach would be not to clamp it at all and simply divide (transect) it (Figure 1). This might seem unconventional, but the aorta is typically occluded, often with thrombus, and can be safely cut with scissors without significant bleeding.
- Aortic Opening: So, the aorta is completely transected in the occluded area without applying an aortic clamp above it (though you should have a clamp ready to close the aorta when removing the thrombus plug). Transect the aorta 2 to 3 cm below the renal arteries and even below the inferior mesenteric artery if possible. After transection, what is next?
- Removal of Thrombus Plug: Plan a thrombectomy around the thrombus using instruments like an endarterectomy spatula, Dunhill clamp, or Mosquito clamp. After mobilizing the thrombus circumferentially, gently press on the aorta with your fingers to squeeze out the thrombus. This is usually successful, and the plug is expelled with the arterial wave pressure, much like uncorking a champagne bottle (Figure 2). At this point, hold the pulsating aorta with your fingers and carefully apply the aortic clamp.
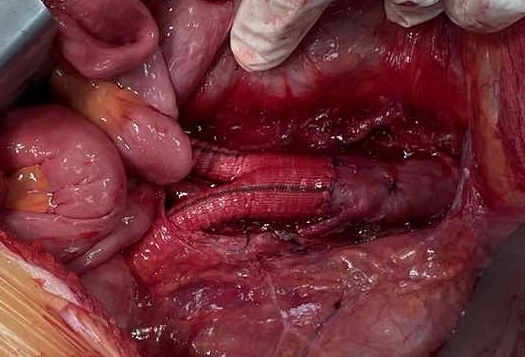
- Next is the aortic graft anastomosis. Since you have transected the aorta, the graft should be placed end-to-end (Figure 3). This approach offers better hemodynamics and reduces bulging protrusions in the limited retroperitoneal space. As for sutures, I prefer using 4/0 Polypropylene with a long, at least 20 mm, ½ curved needle, as opposed to the 3/0 I typically use in AAA open repair.